athenaHealth Scheduling for OB/GYN Practices: A 2026 Operations Guide
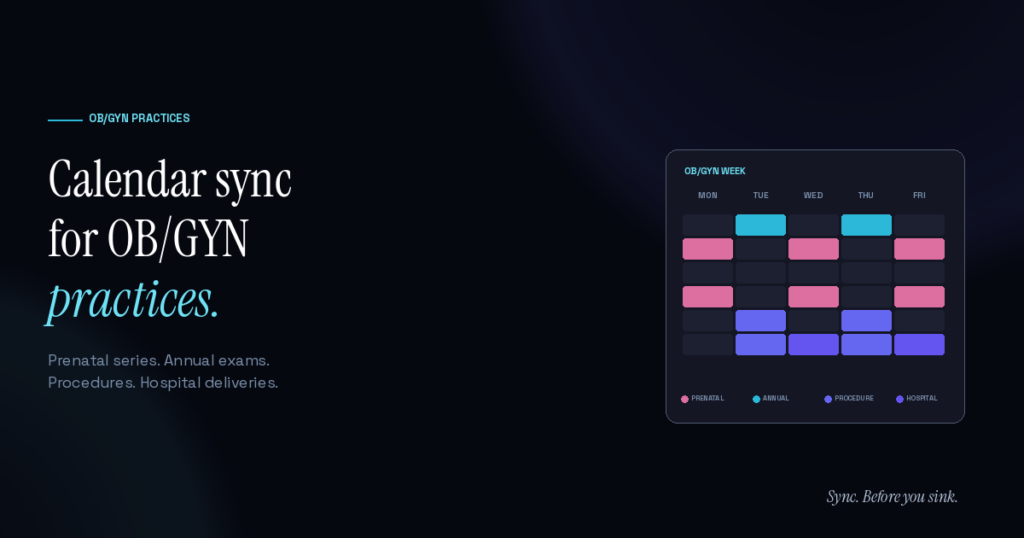
OB/GYN practices on athenaHealth manage a scheduling complexity profile distinct from general primary care: continuous prenatal visit series spanning 9+ months, annual well-woman exams, in-office procedures with longer slot lengths, hospital labor and delivery coverage that pulls providers out of clinic unpredictably, and patient privacy considerations that affect communication patterns. Practice managers running OB/GYN operations smoothly share a few core patterns: dedicated prenatal templates, protected procedure time blocks, hospital-coverage handoffs visible to the front desk, and tight provider availability sync between clinic and on-call schedules.
The stakes are real. OB/GYN patients form long-term relationships with their practice — pregnancy through postpartum, annual exams over decades. A scheduling miss damages a relationship that should generate hundreds of visits over a patient lifetime, not just one missed appointment’s worth of revenue.
What makes OB/GYN scheduling different from general primary care?
The core differences:
- Prenatal series. Each pregnancy involves 12–14 scheduled visits across roughly 40 weeks, with intensifying frequency in the third trimester. The series operates as a continuous booking pattern, not standalone appointments.
- Annual well-woman exams. Most OB/GYN patients see their provider once per year for an annual exam — predictable, recurring, but lower-volume per patient than prenatal patients.
- In-office procedures. Endometrial biopsies, IUD insertions, colposcopies, LEEP procedures — longer slot lengths (45–90 minutes vs. 15–30 for regular visits) with specific instrument and room requirements.
- Hospital labor and delivery coverage. Providers cycle in and out of in-clinic availability based on hospital coverage schedules. A provider on L&D call may need to leave clinic at any moment.
- Patient privacy is heightened. OB/GYN patients have above-average sensitivity to appointment reasons being visible (custody disputes, partner privacy, etc.). Appointment naming conventions and reminder content matter operationally.
According to the American College of Obstetricians and Gynecologists’ practice resources, scheduling reliability directly affects prenatal care quality — missed prenatal visits correlate with worse clinical outcomes, which makes scheduling infrastructure a clinical issue, not just an operational one.
How do prenatal visit series work in scheduling terms?
A standard prenatal series in 2026:
- Initial visit (weeks 6–10): 45–60 minute confirmation visit, history, physical, baseline labs
- Weeks 10–28: Monthly visits, 20–30 minutes each
- Weeks 28–36: Bi-weekly visits, 20 minutes each
- Weeks 36–delivery: Weekly visits, 20 minutes each
- Postpartum (6 weeks post-delivery): 30 minute visit
That’s 12–14 visits over the course of a pregnancy. For a practice managing 50+ active prenatal patients simultaneously, that’s 50+ recurring appointment series running concurrently, each on its own timeline relative to estimated due date.
Practices that handle prenatal scheduling well:
- Use athenaHealth’s recurring appointment functionality for the predictable mid-pregnancy series
- Reserve specific slots for prenatal visits so they don’t compete with other appointment types
- Build in reschedule buffer because pregnant patients reschedule more frequently than the general population
- Tag prenatal patients with their estimated due date for series tracking
How are procedure days handled in OB/GYN practices?
Most OB/GYN practices designate specific procedure days or half-days rather than scattering procedures throughout the week. Reasons:
- Equipment and room turnover. Procedure rooms need specific instruments, prep, and turnover time. Batching procedures reduces setup overhead.
- Provider concentration. Provider stays in “procedure mode” for several hours rather than context-switching between procedures and routine visits.
- Patient prep coordination. Patients prepping for procedures have specific instructions (food restrictions, medication adjustments) that are easier to coordinate when handled in batches.
- Recovery time. Some procedures require post-procedure observation that doesn’t fit between routine visit slots.
Template-wise, this means dedicated procedure blocks (typically 2–3 hours, sometimes a full half-day) that the front desk should never override with routine visits. Template drift on procedure blocks is a common scheduling problem in OB/GYN practices — front desk under pressure books a routine annual into a procedure slot, and the entire procedure day gets compressed.
How does hospital labor and delivery coverage affect clinic scheduling?
The hardest scheduling challenge for OB/GYN practices specifically. When a provider is on L&D call, they may need to leave clinic mid-day to attend a delivery. This is unpredictable — could happen at any moment, could not happen for the whole shift.
Patterns practices use:
- L&D coverage schedules are kept in Google Calendar or a separate scheduling system, not athenaHealth. The clinic schedule doesn’t always know the provider’s on-call status.
- Coverage handoffs between providers require both schedules (clinic + L&D) to be reconciled in real time.
- Backup coverage protocols route patients to a partner provider when the primary is unexpectedly pulled to delivery.
This is exactly the scenario where bidirectional sync between athenaHealth and Google Calendar matters most operationally. If a provider’s L&D call schedule lives in Google Calendar, syncing it back to athenaHealth automatically blocks their clinic slots during call coverage. The front desk sees accurate availability without having to verify call status with the provider before every booking decision.
How should patient communication be handled for OB/GYN specifically?
A few considerations distinct to OB/GYN:
- Appointment names in reminders should be generic. “Appointment with Dr. Smith” rather than “Prenatal visit” or “Contraception consultation.” Reduces privacy risk if reminders are seen by partners or family.
- Confirmation timing matters more. Prenatal series patients sometimes have last-minute pregnancy complications that require schedule changes. Confirmations 24 hours out give the practice time to redirect.
- Telehealth integration. Many OB/GYN visits can be telehealth (counseling visits, results discussions, lactation consultations). The mix between in-person and telehealth affects scheduling differently than primary care.
- Partner involvement varies. Some patients want partners in visits (especially early prenatal); others prefer privacy. The scheduler should ask preference at booking, not assume.
According to the AMA’s 2025 physician AI survey, 57% of physicians prioritize reducing administrative burden through automation. OB/GYN providers specifically benefit because the schedule complexity in their specialty creates above-average administrative load when handled manually.
What metrics matter most for OB/GYN scheduling health?
The specialty-specific KPIs:
- Prenatal visit completion rate. Of scheduled prenatal visits, what percent are attended? Above 95% indicates strong patient engagement; below 90% suggests reminder or access issues.
- Procedure utilization. Percent of procedure-block capacity actually used. Below 75% indicates over-allocated procedure time; above 95% indicates risk of compression issues.
- Same-day access for urgent OB issues. Pregnant patients sometimes need urgent evaluation (bleeding, decreased fetal movement, contractions). Same-day access for these specific reasons is a quality measure.
- Annual exam recall rate. Of patients due for annual exams, what percent are scheduled within 30 days of recall? Below 50% suggests recall workflow issues.
- L&D coverage conflict rate. How often is a provider pulled from clinic to L&D, creating cascading schedule disruption? Track to size the impact on operations.
The general athenaHealth scheduling best practices framework applies too, but the OB/GYN-specific metrics above surface specialty-specific issues earlier.
Frequently Asked Questions
Q: Is athenaHealth a good EHR choice for OB/GYN practices? A: Generally yes, especially for medium-to-large groups. athenaHealth handles the scheduling complexity, has reasonable specialty-specific documentation templates, and integrates with most major lab and imaging providers. Smaller solo practices sometimes prefer OB/GYN-specific EHRs for tighter feature fit.
Q: How should OB/GYN practices handle reschedule frequency? A: Pregnant patients reschedule more frequently than general populations — pregnancy-related symptoms, work disruptions, family logistics. Build template buffer (10–15% of slots held for reschedule absorption) and use waitlists to fill cancellations. The hidden cost of double-bookings and scheduling errors compounds in OB/GYN where prenatal series timing has clinical significance.
Q: What’s the most common OB/GYN scheduling problem? A: L&D coverage conflicts. Providers get pulled to deliveries unexpectedly, clinic schedules don’t reflect on-call status, patients arrive to find their provider isn’t available. The combination of high-stakes clinical context and operational disruption makes this the highest-impact issue to address.
Q: How does telehealth fit into OB/GYN scheduling? A: Multiple visit types are appropriate for telehealth — postpartum check-ins, lactation consultations, contraception counseling, mental health follow-up. Most OB/GYN practices in 2026 run 15–25% of visits via telehealth, slotted within the same athenaHealth template structure with telehealth-tagged appointment types.
Q: Should OB/GYN procedures be scheduled with patients online or via call? A: Most practices reserve procedure scheduling for staff-managed booking rather than patient self-service. Procedures require pre-visit prep instructions, sometimes lab work, and clinical screening that the front desk handles during the booking conversation. Self-service online booking works well for annual exams and routine prenatal visits.
Q: How does Sporo Health work for OB/GYN practices? A: The bidirectional sync between athenaHealth and Google Calendar handles the L&D coverage scenario directly — provider on-call schedules in Google Calendar flow to athenaHealth, marking clinic slots unavailable during coverage. For prenatal series and procedure-day templates, Sporo doesn’t change the athenaHealth-side workflow but ensures the provider’s Google Calendar accurately reflects clinic commitments.
Operational reliability is OB/GYN growth strategy
OB/GYN practices grow through long-term patient relationships. A patient who has a strong prenatal experience often returns for subsequent pregnancies, brings family members, and continues annual care for decades. A patient who experiences a disorganized practice often switches.
The infrastructure layer of operational reliability isn’t glamorous, but it’s where the compounding effect on practice growth lives. For athenaHealth practices managing OB/GYN’s distinct complexity, Sync. Before you sink.
Sporo Health closes the visibility gap that drives most preventable scheduling errors — especially the L&D coverage scenario specific to this specialty.